
It’s axiomatic that child care should promote child development and enhance the capabilities of working parents. Congress can take an important step forward in achieving these goals by reauthorizing the Child Care and Development Block Grant (CCDBG) program, which would expand the type of care available to parents, make child care more affordable to more families, and strengthen families and communities in the process.
CCDBG is an important stream of funding to help states make child care more affordable, particularly for low-income families. States use the grants to fund child care certificate (or voucher) programs for low-income families and for state-decided contracts and grants for care providers. But Congress last reauthorized CCDBG in 2014. Since 2020, annual appropriations have extended it, but a new reauthorization represents a key opportunity to stabilize and improve the program.
In the Senate, the Child Care Modernization Act, S.2828, sponsored by Senator Deb Fischer (R-Neb), would reauthorize the CCDBG program for the fiscal years 2026–2030. Two notable aims of the bill are to empower working parents to make their own decisions regarding the child care services that best suit their family’s needs and to achieve greater child care pluralism by requiring states to maintain a “mixed delivery system.”
The bill would also create a “cost estimation model” to accurately estimate provider grants and increase start-up grants to new providers. This is important in light of evidence suggesting that better cost modeling may be crucial to expanding parental choice by putting center-based and home-based providers on a more equal footing.
Mixed-delivery system and reimbursement rates
Child care takes many forms. Parents may prefer their children to be cared for by relatives, the neighborhood day care, a nanny they’ve been recommended, or at a child care center. A mixed delivery system aims to increase the availability of these different forms of child care. In practice, this would require states to outline how they would use money from the Child Care and Development Fund (CCDF) to expand provider diversity through certifications, contracts, and grants.
Ensuring a mixed delivery system not only increases parental choice but also aligns with parents’ preferences. For example, evidence suggests that parents prefer home-based care for infants and toddlers. However, the most recent Administration for Children and Families (ACF) data, from 2022, shows that 73 percent of children served by state child care certificates received formal center-based care. Even in less regulated states such as Texas and Arizona, only 1 percent of licensed child care spaces are for family or home-based child care (see Figure 1). The majority of their certificates are used at centers. Under the proposed reauthorization, states that historically have given more to center-based providers would be required to show how they intend to diversify their pool of recipients.
Figure 1: Percent of home-based licensed child care spaces
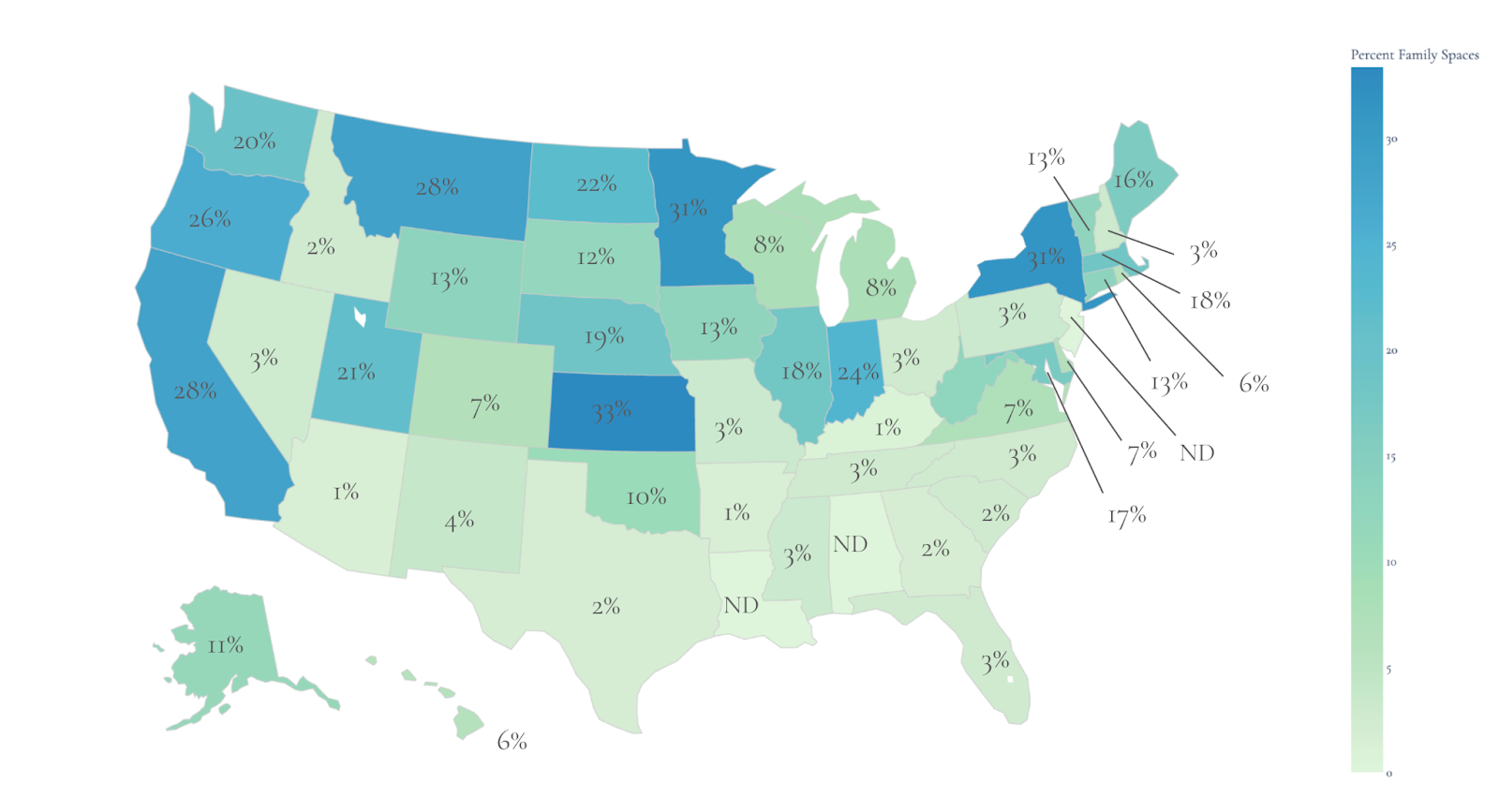
Source: Child Care Aware.
Under the certificate system, certificate recipients (low-income families) give their voucher to a licensed and state-approved provider, who then bills the state for the child’s care, after which the state pays the qualifying provider a reimbursement rate. The reimbursement rate is especially helpful for small, family- and faith-based providers who otherwise might not have the financial flexibility to care for children with vouchers. Ensuring their availability can ensure a better mix of delivery systems.
According to the most recent federal data, at-home providers for children under 5 receive, on average, 70 percent to 80 percent of what their center-based counterparts receive in subsidy reimbursements. Importantly, center-based providers also receive the majority of child care vouchers: on average across all states and territories, 74 percent. And in states such as Texas and South Carolina, center-based providers receive 97 percent to 98 percent of CCDF certificates.
These discrepancies can be explained by the fact that lower reimbursement rates and grants for home-based providers do not accurately reflect labor costs for home-based care. Home-based child care often accommodates parents’ schedules and capacity to pay. Staying open while only serving a portion of the potential children bears a significant labor cost to the provider.
Currently, the ACF relies primarily on state market-rate surveys on child care costs to determine reimbursement rates. These surveys collect data from all formal child care providers on their current prices and operational costs. From these surveys, states then calculate the reimbursement rate, sensitive to the monthly or daily cost of providing care for one child for center-based and home-based providers.
The ACF requires that reimbursement rates be above the 50th percentile of the average child care costs. However, it seems unlikely that the averages from these market rate surveys accurately reflect the true cost home-based providers face. Home-based providers often charge parents what they can pay, making the market rate especially low. Thus, the market rate for at-home care often does not reflect the steep labor costs at-home providers bear.
The Child Care Modernization bill would have states create and use a “cost estimation model” (CEM) instead of market rate surveys to determine more accurate reimbursement rates. Under this model, grants would be calculated to reflect the fixed and operational costs of child care, including staff salaries and benefits, as they differ with the local cost of living. Whether cost estimation models would increase rates for home-based providers and reduce disparities between home-based and center-based providers, potentially incentivizing more of the former, will depend on the details of the model each state decides to use.
Will a cost estimation model increase parental choice?
Whether cost estimation models expand parental choice and provider diversity depend on how a state creates its model and accounts for the labor and regulatory costs of home-based care. New Mexico and Massachusetts have created cost estimation models (or alternative methodologies) to recalibrate payment rates for providers. Until 2021 for New Mexico and 2024 for Massachusetts, these states relied on market rate surveys to calibrate their reimbursement rates.
When New Mexico enacted a CEM in 2022, monthly payment rates increased for every provider and child category. Importantly, the CEM reimbursed home-based providers at a higher rate than center-based providers for toddlers and preschool (by $215 and $125, respectively). One factor driving these changes is that New Mexico’s cost estimation model decouples the reimbursement rate from the rate providers charge private-paying families. Previously, if a provider charged private-paying families a low rate for child care, then the reimbursement rate would reflect that lower rate. This especially harms home-based care providers since they often accommodate their pricing to meet parents’ financial needs, even if these parents do not qualify for a CCDF child care certificate. By decoupling the reimbursement rate from the private-pay rate, home-based care providers, in particular, receive a more robust reimbursement that actually reflects the cost of care.
Table 1: New Mexico reimbursement rates
| Age group | Provider type | Prior monthly rate (FY 2019–2021) | Center v. home gap before | New monthly rate (FY 2022–2024) | Center v. home gap after |
| Infant (6 mo) | Center | $720.00 | $153 | $880 | $5 |
| Family child care | $566.98 | $875 | |||
| Toddler (18 mo) | Center | $589.55 | $126 | $635 | -$215 |
| Family child care | $463.50 | $850 | |||
| Preschool (4 yrs) | Center | $490.61 | $79 | $575 | -$125 |
| Family child care | $411.62 | $700 | |||
| School age (6 yrs) | Center | $436.27 | $29 | $441 | $29 |
| Family child care | $406.83 | $412 |
In Massachusetts (Table 2), all providers received higher reimbursement rates after enactment of an alternative cost estimation methodology. However, the difference between center-based and home-based care reimbursement rose slightly for infant and toddler care.
Table 2: Massachusetts reimbursement rates
| Age group | Provider type | Prior daily rate (2022–2024) | Center v. home gap before | New daily rate (2025–2027) | Center v. home gap before |
| Infant (6 mo) | Center | $79.00 | $30 | $102.07 | $44 |
| Family child are | $48.90 | $58.54 | |||
| Toddler (18 mo) | Center | $69.05 | $20 | $84.70 | $26 |
| Family child care | $48.90 | $58.54 | |||
| Preschool (4 yrs) | Center | $49.91 | $11 | $57.99 | $11 |
| Family child care | $38.90 | $46.50 | |||
| School age (6 yrs) | Center | $43.57 | $5 | $50.62 | $4 |
| Family child care | $38.90 | $46.50 |
Conclusion
By reauthorizing the federal Child Care Development Block program through the Child Care Modernization Act, Congress could make affordable child care more accessible to more parents and families. That would be good for children, families, employers, and society. But success will require the cost-estimation models to focus on promoting diversity in the forms of services provided. Good cost estimation models would need to account for the labor and operational costs of home-based child care. If these costs are not met, CCDF funds would continue to favor center-based providers.




