The Association of American Medical Colleges (AAMC) predicts that there will be a shortfall of as many as 124,000 physicians by 2034. This is the product of two diverging trends: Americans are getting older and their demand for physicians is increasing, while the supply of physicians is shrinking due to retirements and the slow training of new physicians.
The worsening physician shortfall will not impact all Americans equally: underserved communities, such as rural areas, are expected to be hit the hardest. These populations, who already struggle disproportionately with healthcare access and wait times, will see these challenges exacerbated as they have to travel further and wait longer to see a doctor.
The Conrad 30 waiver program–which incentivizes international medical graduates (IMGs) to practice in areas with high medical need –can help address this rural doctor shortage in the U.S. A bipartisan group of senators recently introduced legislation to supplement the Conrad 30 waiver program and increase its benefits for Americans in rural and underserved communities.
Original Conrad 30 Program Overview
Designed by former North Dakota Senator Kent Conrad, the original Conrad 30 waiver program allows states to offer up to 30 waivers allowing IMGs studying in the U.S. on a J-1 visa. The waivers let them skip the two-year foreign residency requirement after graduation if they practice in a medically underserved area or with a medically underserved population.
Since J-1 visas are not dual-intent (that is, they are solely visitor or exchange visas), recipients cannot apply for an immigrant visa, adjustment of status, or an H or L visa automatically after studies are completed. IMGs wishing to remain in the United States must return to their home countries for at least two years before applying for one of these visas, thus experiencing profound disruptions to their personal and professional lives. This is something Conrad 30 waivers for rural U.S. areas with doctor shortages can to address.
Doctors granted Conrad-30 waivers can only practice in areas within federally designated categories, such as Medically Underserved Areas (MUAs) or Health Professional Shortage Areas (HPSAs). Recipients may also work specifically with a Medically Underserved Population (MUP). The program is a needed boost for rural areas of the U.S. experiencing doctor shortages, as only 1% of doctors in their last year of medical school say they want to live in communities under 10,000, and 2% want to live in towns of 25,000 or fewer.
States are also granted significant authority in managing the program, from approving applicants to determining how they are geographically distributed. They can also approve up to 10 “flex” applicants who do not work in a federally designated area of need but meet shortage criteria set by the state and reserve specific slots in their waiver pool for specialists.
Stringent job protections for Americans are also built into the program. While states oversee the specific requirements of what an employer applying for a Conrad 30 waiver needs to demonstrate, they must generally attest that they have been unsuccessful in recruiting a U.S. physician for the same position.
Strengths
Over the past 15 years, the program has brought over 15,000 physicians to areas and patients with significant medical needs. Using a conservative estimate from a study on patient panel sizes translates to at least 44 million patients treated by a Conrad 30 doctor since the start of the program.
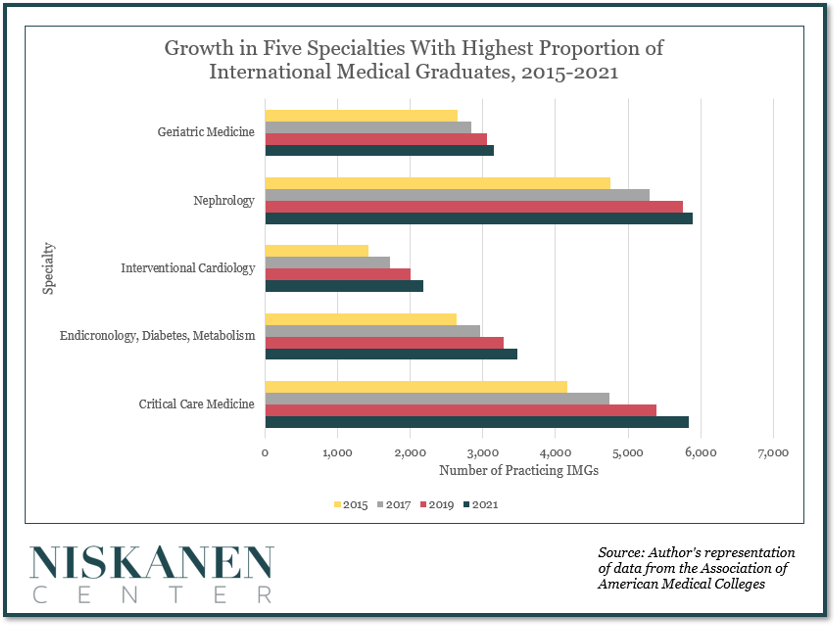
IMGs are also disproportionately concentrated in areas with anticipated shortages. For example, they accounted for over 50% of geriatric medicine practitioners in 2021. As the share of older Americans continues to increase, the need for these specialists will also grow just as their numbers are expected to diminish. IMGs are also highly represented in essential fields such as kidney diseases, interventional cardiology, diabetes care, and critical care medicine. The concentration of likely Conrad 30 recipients in these fields demonstrates how necessary the program is for these specialties.
The program also touts promising completion and retention rates in rural areas with doctor shortages. A 2018 Iowa-based study found that 92% of Conrad 30 recipients in the state met their original three-year obligation and 68% were retained beyond their required time frame.
Challenges
Because of the program’s decentralized nature, collecting standardized, regular data on its status and outcomes is challenging, making it difficult to offer suggested improvements.
One study, however, did report anecdotal doubts that the program facilitates integration, attributing this to the high-stress environments of many designated areas, their isolated locations, and the limited duration of the service period.
Furthermore, the full breadth of issues affecting rural communities and challenges within the U.S. healthcare system sit well outside the scope of this one narrow immigration program, and its impact, while important, remains limited (for more work from Niskanen on healthcare policy, see here and here.)
Conrad State 30 and Physician Access Reauthorization Act
The primary vehicle for Conrad 30 reform in recent years is the Conrad State 30 and Physician Access Reauthorization Act. It was recently re-introduced with broad bipartisan support, including from Republicans in rural states like Senator John Thune of South Dakota, Senator Shelley Moore Capito from West Virginia, and Senator John Boozman from Arkansas.
The bill — which has also garnered support from several key healthcare associations, including the American Medical Association, the National Rural Health Association, and the American Hospital Association — significantly improves the Conrad 30 program by further addressing rural doctor shortages and overhauling the program’s weaknesses.
First among these is the reauthorization and extension of Conrad 30 for three more years, enabling current medical students and potential employers to better (and more definitively) set long-term plans.
It also increases the number of slots for every state from 30 to 35–provided that 90 percent of the waivers available to the states receiving at least five were used in the previous fiscal year. Waiver spots continue to increase by five under this metric, with the threshold being increased to 95% once the number reaches 45 waivers. Increases would be maintained unless waivers granted decrease by 5%.
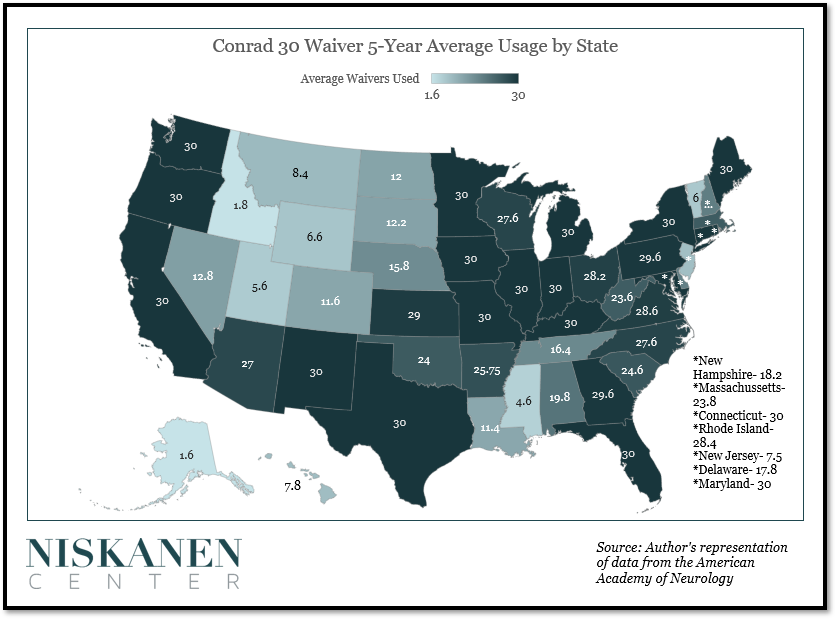
This update is particularly timely, as the U.S. population had increased significantly since 2003, when the original 30 spots-per-state allocation was established. What’s more, recent data indicates that most states used 90% or more of their available waivers, demonstrating the necessity of this provision.
The bill strengthens worker protections, as organizations seeking to employ Conrad recipients must disclose the number of working hours, level of compensation, and other benefits recipients could receive during their time there. Recipients would also now be able to switch locations if they are subject to workplace violations, and states that lose spots to these departures would be able to recapture lost waivers.
The dual intent issue raised by J-1 visas would be addressed by clarifying that expressing interest in receiving a future Conrad 30 waiver does not make an applicant ineligible. Finally, the bill mandates a yearly report on Conrad 30 usage to Congress, which will help remedy the existing data gap on the program.
Conclusion
When operating as intended, the Conrad 30 program helps rural U.S. areas experiencing doctor shortages and gives many IMGs a chance to thrive in America, benefiting all parties involved. Patients who may otherwise have had no recourse but to wait months or years to receive medical attention gain improved access to local healthcare. Employers who manage understaffed practices in locations typically unattractive to recent medical graduates obtain an invaluable new employee pool. And international medical graduates who would otherwise need to upend their lives can stay in the United States and are granted increased stability and security in their personal and professional lives.
The Conrad 30 Reauthorization bill offers a rare opportunity for policymakers to take action on something unilaterally benefiting all parties involved. In passing the bill, policymakers will strengthen the conditions necessary for the aforementioned outcomes to come to fruition while signaling that the program’s myriad benefits transcend partisanship.