This work was produced in collaboration with the Partnership for Innovation, Cross-Sector Collaboration, Leadership, and Organization (PICCLO), School of Arts and Sciences, University of Pennsylvania.
When COVID-19 first struck, many observers looked with dread toward its likely impact on poor countries. With fragile and often corrupt governments, weak public health systems, and inadequate medical resources, these nations seemed defenseless against the novel coronavirus. “The pandemic will have dramatic consequences, eroding many of the gains recorded over the last decade in terms of poverty reduction,” predicted a working paper from the World Institute for Development Economics Research.
As the months passed, however, a more ambiguous picture began to emerge. Writing in the New Yorker in early 2021, Siddhartha Mukherjee described what he called an “epidemiological mystery.” Going by reported death rates, many poor countries like India and Nigeria seemed to be coping with the pandemic not less but more successfully than rich countries like Italy, Belgium, or the United States. Why could that be?
Mukherjee concluded that underreporting of infections and deaths in countries with weak statistical systems was only part of the explanation. Other factors seemed to be at work, too, including differences in the age structure of populations, prior exposure to infectious diseases, and differences in living arrangements. Finally, some of the experts that Mukherjee consulted emphasized that pandemic outcomes also depended on differences in the effectiveness with which governments responded to the crisis.
The following discussion will focus on this last aspect of the epidemiological mystery: the effectiveness of the government response as measured by an index of state capacity. Here, as in previous work, the index of state capacity is based on data provided by the Legatum Institute as part of its annual Legatum Prosperity Index. Specifically, state capacity is construed as the ability of a government to formulate and carry out policy goals (administrative capacity); to provide security against crime and external enemies (security capacity); and to manage government finances (fiscal capacity).[1]
Measures of pandemic outcomes are based on research reported in two articles published in the British journal The Lancet, which provide country data on pandemic outcomes in the form of infection rates and mortality rates.[2] The studies provide infection rates in both an unadjusted version, as publicly reported, and a version that is adjusted for a variety of demographic, economic, and epidemiological factors. In addition to unadjusted mortality rates, the second Lancet study provides an estimate of excess mortality, that is, an estimate of the amount by which a country’s overall mortality rate, adjusted for underreporting, exceeds what would have been expected if there had been no pandemic.
A two-factor model of state capacity and pandemic performance
Simple correlations of state capacity with infection and mortality rates do not yield much of interest. There are small tendencies for reported infection rates to fall and for reported mortality rates to rise with increasing state capacity. However, the correlations of state capacity scores with all four outcome variables lie below the threshold of statistical significance. But simple correlations can hide more than they reveal. Closer examination of the data shows that there are significant nonlinear relationships between state capacity and pandemic outcomes.
Figure 1 illustrates the nonlinear relationship in the case of unadjusted infection rates. Data on both axes are standardized to show the number of standard deviations by which each observation falls above or below a mean value of zero for that variable. The arched trendline shows a tendency for reported infection rates to be highest in countries with state capacity scores near the mean, while these infection rates tend to be lowest for countries with very high or very low state capacity scores.
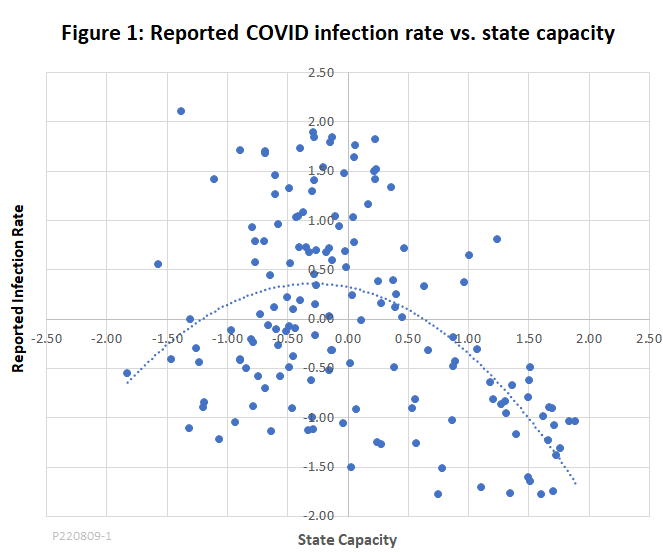
The fit of the curve with the data is not exact, but it meets a test of statistical significance with room to spare.[3] Similar significant nonlinear correlations are found for adjusted infection rates and for both reported mortality and excess mortality rates. But these patterns are little more than curiosities unless they can be explained in terms of some credible causal model.
One credible model is based on the interactions between two types of causal factors that jointly determine pandemic outcomes. Those that are associated with lower infection or mortality rates as state capacity increases will be called facilitating factors, since they facilitate an effective response to the pandemic. Others that are associated with higher infection or mortality rates as state capacity rises will be called contravening factors since they are contrary to the expectation that countries with greater state capacity should be better able to deal with pandemics. In this two-factor model, the overall success of a country’s response to the pandemic would potentially depend both on the individual facilitating and contravening factors and on the way they interact.[4]
The facilitating factor that is most widely discussed in the literature is the quality of a country’s health care and public health systems. Here, those are measured by the average of the Legatum Institute’s compound variables “Care Systems” and “Preventive Interventions.” Each of the Legatum elements correlates strongly with state capacity (R = 0.86 and R = 0.65, respectively.) We should expect the quality of health care and public health systems to increase with increases in overall state capacity, and thus for higher state capacity to be associated with better pandemic outcomes.
Contravening factors, meanwhile, push in a counterintuitive direction: When these factors are in play, we should expect increases in state capacity to be associated with worse outcomes. Two of the most widely discussed contravening variables are the accuracy with which infection and mortality rates are reported in a given country and the country’s population age structure. Countries with very low state capacity will be unable to track cases and deaths accurately. Accordingly, as state capacity rises from low levels, we should expect to see reported cases and deaths rise because of better tracking and reporting, and that is just what happens. Also, countries with low state capacity tend to be poor, with relatively young populations. Since cases and deaths are generally much lower among young people, we should expect the countries at the bottom of the state capacity rankings to have better outcomes as a result of their population structure. As we move to countries with higher state capacity, we are looking at countries with older populations and should expect worse outcomes.
The data support all of these expectations regarding the relationship of state capacity to the facilitating and contravening factors. The ratio of reported mortality to excess mortality reported in the March 2022 Lancet study cited above was used as an estimate of reporting accuracy for both mortality and infection rates. The accuracy ratio is positively and significantly correlated with state capacity (R = 0.69). Population age structure was represented by old-age dependency ratio (ratio of population aged 65 and older to the working-age population) provided by the World Bank. The old-age dependency ratio, too, is strongly correlated with state capacity (R = 0.75). Old-age dependency is a contravening factor since, other things being equal, an older population is more vulnerable to COVID-19. For this study, the contravening factor in the two-factor model was represented by the average of the standardized values of reporting accuracy and old-age dependency.
The two-factor model produces statistically significant results for all four measures of pandemic outcomes. The results are strongest when the model is applied using reported death rates as the response variable (R = 0.74), but the multiple correlations are also significant for excess mortality and for both reported and adjusted infection rates. These results are consistent with the hypothesis that state capacity has multiple effects on pandemic outcomes, including both facilitating effects resulting from better health systems and contravening effects resulting from reporting accuracy and population age structure.
Is state capacity just a proxy for high income?
One more issue needs to be raised to round out the analysis. Countries with high state capacity, for the most part, tend also to have high per capita incomes. To the extent that those countries have better pandemic outcomes, how do we know that is specifically because they are well governed, and not just because they are rich?
Statistically, the correlation coefficient between state capacity and gross national income (GNI) per capita is a strikingly high 0.87 for the 152 countries covered by this study. That is not really surprising, considering that there are strong causal connections between good government and high incomes. What is more, the causal connections operate in both directions. Higher national income provides the resources needed to run an effective government – to educate civil servants, pay them enough to resist the temptations of petty corruption, build infrastructure and so on. At the same time, better government facilitates economic growth by maintaining law and order, supporting orderly markets, and providing good public services.
However, the fact that state capacity and national income are highly correlated does not mean they are interchangeable. Two variables are statistically interchangeable only if neither of them contains substantively important information that the other does not. For example, suppose we have two measurements of the temperature in a certain city based on two thermometers. Neither of the instruments is perfectly accurate. Each gives the same average temperature over time, but the reading from each instrument on any given day is equal to the true temperature plus a small random error. The temperature readings from these two thermometers would not only be highly correlated, but would be fully interchangeable in that neither would give a different answer to a question such as whether it is more likely to rain on warm days or cool days.
One way to explore the interchangeability of two variables is to look not just at their correlation, but at their outliers. The outliers are cases where the two variables do not line up – for example, days or weeks in which the readings of Thermometer A are higher than those from Thermometer B. If the outliers are random, we would not expect the average rainfall in those weeks to be significantly different from the rainfall in weeks where Thermometer B gave higher readings than Thermometer A.
Returning to the subject of this study, the outliers are countries for which state capacity is higher or lower than expected predicted by per capita income. If state capacity and income were interchangeable, we would find no discernable pattern in the outliers. For example, we could ask whether mortality rates are significantly different from those predicted by the two-factor model in countries in which state capacity is different from what is predicted by income.[5] If patterns were found, we could begin to look for explanations. Does state capacity influence pandemic performance more strongly than does per capita income? Are there other variables that explain the reasons for the nonrandom factors that are observed?
As it turns out, for the full sample of 152 countries, there is no significant tendency for countries with higher-than-expected state capacity to have higher- or lower-than-expected mortality rates. However, if we look at the results for regional groupings of countries, some interesting patterns emerge.
For example, in the East Asia and Pacific region, state capacity averages 25 points higher than would be expected based on the region’s average income.[6] At the same time, reported mortality rates in that region are 78 points lower and excess mortality rates are 91 points lower than predicted by the two-factor model. A similar pattern, although not as strong, is found in Central and South Asia, and again, although weaker, in Western Europe and North America. These findings suggest that when these regions are compared with global averages, higher state capacity has a favorable impact on pandemic outcomes above and beyond any effect produced by differences in income alone.
Meanwhile, in Latin America and the Caribbean, the average score for state capacity is 10 points below the level that is expected based on income, while reported and excess mortality are higher than predicted by the two-factor model. Here, low state capacity appears to have the effect of raising mortality rates above what would be expected from income alone.
Eastern Europe, however, provides a contrasting example. Eastern European countries have lower average per capita GNI than those in Western Europe, but their state capacity is nevertheless somewhat higher than expected based on income alone. Surprisingly, though, in that region reported and excess mortality rates are higher, not lower, than is predicted by the two-factor model. It is interesting to speculate as to why.
One possible explanation is suggested by previous studies that have shown that high levels of social and political trust have favorable effects on pandemic outcomes above and beyond the effects that are accounted for by the two-factor model.[7] Both social and political trust are substantially higher than the world average in East Asia. In that region, high trust appears to reinforce the favorable effect of state capacity on pandemic mortality rates. On the other hand, both social and political trust are much lower in Eastern than Western Europe. In Eastern Europe, it may be that the large deficit of trust more than offsets the favorable effect of state capacity that is somewhat higher than expected based on income.
The so-called petrostates are another group of countries for which state capacity scores depart widely from those predicted on the basis of income. Consider Iraq, whose oil exports contribute 32 percent of GDP, which, according to World Bank data, is the highest oil export share of any country. Iraq’s state capacity score is 57 points below what would be predicted based on income. At the same time, the country suffered terribly from the COVID-19 pandemic, experiencing an excess death rate 99 points higher than predicted by the two-factor model. However, that pattern of low state capacity linked to high mortality rates is not found consistently across oil-rich countries. For example, Saudi Arabia, like Iraq, has a state capacity score well below the predicted level, but its excess death rate from COVID was below, rather than above, the level predicted by the two-factor model. Across 18 countries that have oil exports in excess of 5 percent of GDP, state capacity averages 38 percent of what would be predicted on the basis of income, yet average excess death rates for these petrostates are not significantly different from the world average.
Taken together, these examples show that income and state capacity, although highly correlated, are not interchangeable. And for many countries and groups of countries, the pandemic outcomes implied by income alone differ greatly from those implied by state capacity scores. The reason, presumably, is that many other factors are at work in determining pandemic outcomes, including aspects of social capital, such as trust; economic factors, such as dependency on resource exports; cultural factors, such as kinship structures; and epidemiological factors, such as prior exposure to infectious diseases. All of these deserve further investigation.
Overall, the evidence examined here remains consistent with the hypothesis that countries that are well-governed have weathered the COVID-19 pandemic better than those that are not. But many puzzles remain regarding other factors beyond state capacity that have determined pandemic outcomes around the world.
1 Administrative capacity is measured by the Legatum element for government effectiveness; security capacity by the Legatum elements for war, terrorism, and crime; and fiscal capacity by the Legatum indicator for country credit rating. The administrative, security, and fiscal components are equally weighted to get the overall state capacity index.
2 The Lancet, “Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021,” February 01, 2022 (doi.org/10.1016/S0140-6736(22)00172-6) and The Lancet, “Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020–21,” March 10, 2022 (doi.org/10.1016/S0140-6736(21)02796-3).
3 When the reported infection rate is used as the response variable and state capacity and the square of state capacity are used as the response variable, the coefficient of multiple correlation is 0.52. The multiple correlation and the coefficients on each of the control variables are significant at the 0.01 level.
4 Mathematically, the two-factor model can be represented as R = FF + CF + FF*CF, where R is the outcome being measured (case rate or mortality rate), FF represents one or more facilitating factors, CF represents one or more contravening factors, and FF*CF, the product of FF and CF, represents the interactive effect. For a more detailed discussion of the two-factor model, see “Trust, State Capacity, and the Epidemiological Mystery of Covid,” Niskanen Center, April 28, 2022. That paper includes a link to the underlying data used in this study and details of key statistical results.
5 In the language of statistics, the question can be posed in terms of residuals. Define a country’s state capacity residual as the number of standard deviations that its observed state capacity exceeds or falls short of the value that would be predicted by its GNI per capita. Similarly, define its excess or reported mortality residual as the number of standard deviations by which its observed excess or reported mortality rate exceeds or falls short of the value predicted by the two-factor model. If income and state capacity are interchangeable, we would expect to find no statistically significant patterns in the mortality residuals and state capacity residuals.
6 “Points” is used here as shorthand for hundredths of a standard deviation on the standardized scale used in Figure 1. See Appendix Table 1 for the full data.
7 See, for example, the February 2022 Lancet study cited in note 2 and the Niskanen Center commentary cited in note 4.
Photo Credit: iStock